Topical Steroids: How to Prevent Skin Thinning and Use Them Safely
 May, 31 2026
May, 31 2026
It is a common fear in dermatology circles. You are prescribed a cream for your eczema or psoriasis, but you worry that using it will permanently damage your skin. The phrase "skin thinning" sounds terrifying, leading many patients to underuse their medication or stop it entirely. This hesitation often causes more harm than the medicine itself. Topical steroids are medications applied directly to the skin to reduce inflammation and treat conditions like eczema, psoriasis, and dermatitis. When used correctly, they are safe, effective, and rarely cause serious side effects. The key lies in understanding potency, dosage, and duration.
These medications have been the cornerstone of outpatient dermatology since the early 1950s. According to data from the Practicing Clinicians Exchange (2023), they remain the most commonly prescribed treatments by dermatologists. While misuse can lead to complications like atrophy (thinning of the skin), proper use minimizes these risks significantly. Let’s look at how to use them without damaging your skin barrier.
Understanding Potency Classes
Not all steroid creams are created equal. Topical corticosteroids are classified into seven categories based on their strength, ranging from super-potent (Class I) to low-potency (Class VII). Using a Class I steroid on your face is like using a sledgehammer to crack a nut-it is unnecessary and dangerous. Conversely, using a Class VII steroid on thick plaque psoriasis on your elbows might do nothing at all.
The American Academy of Family Physicians (2021) highlights that the vehicle type also impacts potency. Ointments are the most potent because they are occlusive, trapping moisture and driving the medication deeper into dry, thickened skin. Creams are next in line and work well for moist or weeping lesions. Gels and lotions are better suited for hair-bearing areas or flexural zones (like behind the knees), while foams are cosmetically acceptable for the scalp.
| Potency Class | Strength Level | Recommended Body Areas | Duration Limit |
|---|---|---|---|
| Class I - III | Super-Potent / Very Potent | Palms, soles, thick plaques | Max 2 weeks |
| Class IV - V | Moderately Potent | Trunk, limbs (avoid face) | 2-4 weeks |
| Class VI - VII | Low / Mild Potency | Face, groin, underarms, eyelids | Up to 4 weeks |
The GOV.UK guidance (2023) emphasizes that only mild potency products should ever be used on sensitive areas such as the face (especially eyelids), groin, and underarms. Stronger formulations are reserved for thicker-skinned areas like the palms and soles. Matching the right strength to the right location is the first step in preventing skin atrophy.
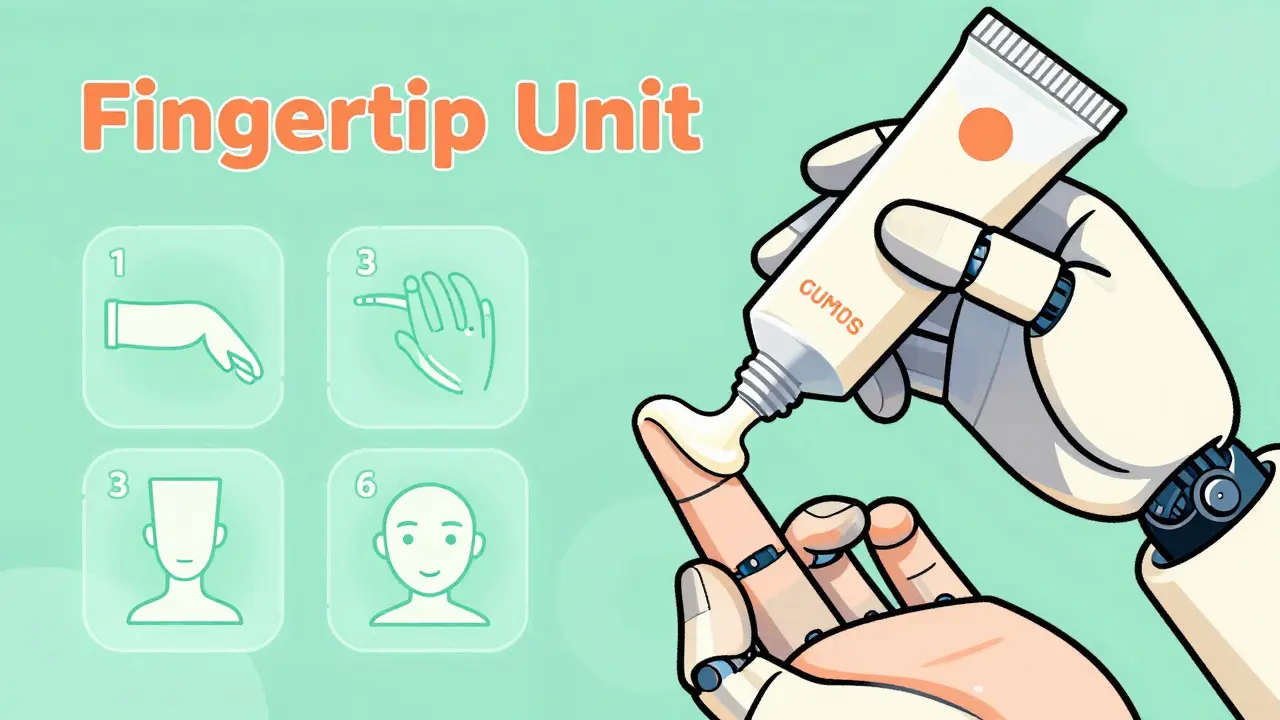
The Fingertip Unit Rule
One of the biggest reasons people develop side effects-or fail to see results-is incorrect dosing. Patients often apply too little, which prolongs the flare-up, or too much, which increases absorption and risk. The solution is the Fingertip Unit (FTU) is a standardized measure of medication quantity squeezed from a tube between the tip of the index finger and the first crease.
There is some variation in standards. The Practicing Clinicians Exchange (2023) states one FTU equals approximately 0.25 grams, while NIH StatPearls (2023) indicates it can be up to 0.5 grams depending on the tube diameter. Regardless of the exact gram weight, the visual rule remains consistent. Squeeze the tube until the strip of cream covers your adult index fingertip to the first joint.
- One hand (front and back): Needs 1 FTU.
- One arm: Requires 3 FTUs.
- One leg: Requires 6 FTUs.
- One foot: Needs 2 FTUs.
The American Academy of Family Physicians (2021) notes that a small amount goes a long way. Rub the medication gently onto the affected area until it is absorbed. Do not layer it heavily. If you run out of cream before covering the area, you likely started with too little. If you have half a tube left after treating one arm, you used too much.
Application Frequency and Timing
How often should you apply the cream? For super-potent to moderately potent corticosteroids (ranks 1-4), once daily application is sufficient. For potent to low-potency formulations (ranks 5-7), twice-daily application is recommended according to This Changed My Practice (2023). Applying more frequently than prescribed does not speed up healing; it only raises the risk of adverse effects. The AAFP (2021) explicitly states there is no beneficial evidence for applying topical corticosteroids more than once daily for atopic dermatitis.
Timing matters when combining steroids with moisturizers (emollients). Many patients apply their moisturizer and then the steroid immediately after. This dilutes the steroid’s effectiveness. Both GOV.UK (2023) and NIH StatPearls (2023) advise waiting 20-30 minutes between applications. Apply the steroid first to clean, dry skin, let it absorb, and then apply your emollient later to lock in moisture. Alternatively, you can apply the emollient first, wait 20 minutes, and then apply the steroid. Consistency is key.
Skin Thinning: What Really Happens?
Skin atrophy is the medical term for skin thinning. It occurs when collagen production decreases due to prolonged exposure to high-potency steroids. Symptoms include visible blood vessels (telangiectasia), easy bruising, and striae (stretch marks). However, this is largely preventable.
The National Institute of Health's StatPearls (2023) documents that high-potency steroids should not be administered for longer than two weeks. Total treatment duration for any potency should generally not exceed 2-4 weeks without medical review. Dr. Jonathan Silverberg, referenced by the National Eczema Society (2023), recommends a "step-down" approach. Start with a strong steroid to get symptoms under control quickly, then switch to a lower strength steroid or non-steroidal alternative to maintain remission.
Facial application carries unique risks. The Arthritis Foundation (2023) highlights that facial use may cause perioral dermatitis (a red rash around the mouth) or acne-like eruptions. Prolonged use near the eyes can contribute to cataracts or glaucoma. If you need treatment for facial eczema, ask your doctor about non-steroidal alternatives like calcineurin inhibitors (e.g., tacrolimus or crisaborole), which do not cause skin thinning.
Common Mistakes to Avoid
Patient experiences reveal several recurring errors. First, self-treating chronic eczema with high-potency steroids for months without supervision. Reddit discussions cited in community forums describe cases where individuals developed visible thinning and stretch marks in flexural areas due to unsupervised long-term use. Second, under-applying the medication. The GOV.UK guidance (2023) explains that using too little steroid can prolong treatment time and paradoxically increase the risk of side effects because the condition stays inflamed longer.
Another mistake is ignoring withdrawal reactions. Some patients develop rebound flares after stopping steroids abruptly. Tapering off the medication or switching to a milder formulation helps mitigate this. Finally, do not ignore signs of infection. Steroids suppress local immune responses. If your skin becomes hot, painful, or oozes pus, stop the steroid and seek medical advice, as you may have a secondary bacterial or fungal infection.
Alternatives and Future Directions
If you are concerned about skin thinning, you are not alone. The market is shifting toward safer options. Non-steroidal alternatives like crisaborole and tacrolimus are increasingly prescribed for facial and sensitive area treatment, though cost can be a barrier. Research published in the Journal of Investigative Dermatology (March 2023) explores novel delivery systems that target inflammation while minimizing epidermal thinning. These technologies aim to deliver the active ingredient deeper into the dermis without affecting the epidermis where thinning occurs.
Despite these advancements, topical corticosteroids remain essential. The American Academy of Dermatology’s 2023 position statement emphasizes that when used appropriately under medical supervision, the benefits significantly outweigh the risks. The future is not eliminating topical steroids but using them smarter. By following strict protocols regarding potency, duration, and dosage, you can manage your skin condition effectively without compromising its integrity.
How long does it take for skin thinning to reverse?
Mild skin thinning often reverses within a few months of stopping the offending steroid. However, severe atrophy with striae (stretch marks) or permanent vascular changes may not fully resolve. Prevention through proper usage is far more effective than reversal.
Can I use topical steroids on my face?
Yes, but only mild-potency steroids (Class VI or VII) and for short durations (no more than 5-7 days). Avoid using stronger steroids on the face, especially near the eyes, due to the risk of glaucoma, cataracts, and perioral dermatitis.
What is the difference between a cream and an ointment?
Ointments are oil-based and more occlusive, making them more potent and better for dry, thickened skin. Creams are water-based, less greasy, and suitable for moist or weeping lesions. Choose the vehicle based on your skin type and lesion characteristics.
Should I moisturize before or after applying steroid cream?
Apply the steroid first to clean, dry skin, then wait 20-30 minutes before applying moisturizer. This ensures the steroid is absorbed properly and not diluted by the emollient.
Are topical steroids addictive?
Topical steroids are not chemically addictive. However, psychological dependence or "steroid phobia" is common. Additionally, abrupt cessation after long-term use can cause rebound flares, which some mistake for addiction. Always taper under medical guidance.